
In this article five important things to know about extended spectrum beta-lactamases (ESBL) are identified by a clinical microbiologist.

Authored By: Jose Alexander, MD., D(ABMM), FCCM, BCMAS, SM, MB(ASCP)
A special recognition and appreciation to Amy Carr, PharmD, BCIDP for her contribution and to this article.
Last updated: 28 November 2020
1. If the Microbiology laboratory does not report ESBL, how do I recognize an ESBL organism?
Since 2010, the Clinical and Laboratory for Standards Institute (CLSI) M100 Performance Standards for Antimicrobial Susceptibility Testing has stated “when using the current breakpoints, routine ESBL testing is no longer necessary before reporting results.” Therefore, many laboratories do not routinely perform ESBL screening or confirmation anymore. In addition, it is no longer necessary to edit the results for penicillins, cephalosporins, and aztreonam from susceptible to resistant for confirmed ESBL isolates. However, ESBL testing may still be useful for epidemiological or infection prevention purposes.
Although laboratories that have implemented CLSI breakpoints after 2010 are not required to routinely test for ESBL, most are still able to perform screening or confirmatory testing.
My recommendations:
- Discuss with your microbiology laboratory and understand current testing protocols for Enterobacterales, especially the role of the ESBL testing when third generation cephalosporin (3GC) and fourth generation cephalosporin (4GC) are intermediate or resistant. It is important to also understand the role that Infection Prevention plays in this regard, especially since some facilities may require isolation to be implemented for patients with ESBL infections.
- Extended Spectrum Beta-Lactamases can still be evaluated and deduced based on the phenotypic susceptibility of the MIC distribution. The susceptibility result provided by the laboratory may show a characteristic pattern of an ESBL.
2. What are the criteria for confirming an ESBL?
Based on the CLSI M100 standards, ESBL screening and confirmation is indicated only for Escherichia coli, Klebsiella pneumoniae, Klebsiella oxytoca, and Proteus mirabilis.
The most common method of ESBL confirmation is the phenotypic double-disk diffusion method (see image below) based on the inhibition of clavulanic acid over the ESBL enzyme recovering the activity of cefotaxime and/or ceftazidime. If the activity of either one of these two 3GC is recovered by clavulanic acid, then the presence of an ESBL is confirmed. Although the recovering of only one 3GC is required, it is recommended to test both agents with and without clavulanic acid to improve the sensitivity of this method. This technique is based on the principles that ESBL enzymes are inhibited by clavulanic acid and evidence of restored activity of the cephalosporin by this inhibitor indicates the presence of this resistance mechanism.
There is also molecular confirmation of ESBL, and this is based on detection of the ESBL gene. CTX-M is the most common and wide-spread ESBL gene in multiple regions, including North America. A small percentage of ESBL are caused by broad-spectrum enzymes coded by SHV/TEM ESBL-genotypes. Detection of the CTX-M gene is commonly limited to rapid blood culture polymerase chain reaction (PCR) identification methods which include this gene as part of the routine screening of positive blood cultures. SHV/TEM ESBL genes detection by PCR or other molecular method is not currently available for clinical use.

Image 1. The inhibition zone around cefotaxime & ceftazidime with clavulanic acid, and the absence of inhibition around the same agents with cloxacillin, demonstrate the presence of an ESBL.
3. Are all resistances of Enterobacterales against 3GC caused by ESBL?
No, some of the 3GC resistant organisms are AmpC producing, but almost all resistance against 3GC on Enterobacterales are beta-lactamase mediated.
When dealing with Enterobacterales it is important to differentiate 2 major groups. E. coli, K. pneumoniae, K. oxytoca & P. mirabilis are the group that lack intrinsic resistance to extended spectrum cephalosporins. Their wild-type beta-lactam pattern is considered pan-susceptible except for K. pneumoniae and K. oxytoca that are resistant to ampicillin by the presence of plasmid-mediated TEM/SHV.
The second group, commonly referred to as SPiCE or SPiCE-M, includes Serratia marcescens, Providencia stuartii, Citrobacter spp., Enterobacter spp., and Morganella morganii. These organisms (except for some species in the Enterobacter and Citrobacter genera) carry a chromosomal cephalosporinase commonly referred as AmpC. This group of genes belongs to the Ambler Class C and they are not inhibited by clavulanic acid, sulbactam or tazobactam (with some exceptions). The spectrum of activity for AmpC does not include cefepime.
It is important to recognize that SPiCE-M organisms can show a susceptible or resistant pattern against 3GC as wild-type and this is the result of having a regulated chromosomal AmpC. It should be assumed, even when susceptible, that expression of AmpC could occur during a treatment course with beta-lactams. The presence of AmpC makes it difficult to differentiate resistance secondary to an ESBL or an AmpC. This is one of the reasons that there are not routine screening protocols for ESBL on SPiCE-M organisms. An ESBL screening method using phenotypic double-disk diffusion of cefepime with clavulanic acid is available against organisms that co-produce AmpC. Screening for AmpC using cloxacillin as the AmpC inhibitor is also available and recommended by the EUCAST (European Society of Clinical Microbiology and Infectious Diseases) Guidelines for Detection of Resistance Mechanisms and Specific Resistances of Clinical and/or Epidemiological Importance.
4. How can I recognize the presence of an ESBL or AmpC from the susceptibility report of Enterobacterales?
Evaluating the MIC distribution and breakpoints of cefoxitin, cefotaxime/ceftriaxone, ceftazidime, and cefepime may guide clinically meaningful recognition of the resistance mechanism with potential to impact therapeutic decision making. The principles are based on the spectrum of activity of an ESBL compared to an AmpC as well as the Enterobacterales species.
Let’s start some basic rules:
- Screening and detection of ESBLs focuses on E. coli, K. pneumoniae, K. oxytoca, and P. mirabilis. This group of organisms do not carry intrinsic resistance against 3GC, 4GC or cefoxitin.
- All ESBLs are acquired resistance mechanisms. ESBL hydrolyze 3GC and 4GC, but do not hydrolyze cefoxitin. ESBLs are inhibited by beta-lactamase inhibitors – clavulanic acid, sulbactam, & tazobactam.
- AmpC is also an acquired resistance in E. coli, K. pneumoniae, K. oxytoca, and P. mirabilis. AmpC is not inhibited by clavulanic acid, sulbactam, or tazobactam, but it may be inhibited by cloxacillin (new available inhibitors as avibactam and relebactam also have inhibitory activity). AmpC has a high affinity to hydrolyze cefoxitin but not cefepime which results in AmpC being cefoxitin resistant and cefepime susceptible.
- From an Infection Prevention perspective, AmpC has the same epidemiological importance as an ESBL, it is because AmpC is a plasmid-mediated acquired resistance (except for some E. coli with derepressed chromosomal AmpC) and could require isolation based on facility’s polices
How to evaluate which beta-lactamase (ESBL vs. AmpC) is present for an E. coli, K. pneumoniae, K. oxytoca, or P. mirabilis based on susceptibility report:
Step 1: Review susceptibilities of 3GC to confirm the presence of an Extended Spectrum Beta-Lactamase.
- Ceftriaxone or cefotaxime MIC 2 mcg/mL (intermediate or resistant)
AND/OR
- Ceftazidime MIC 8 mcg/mL (intermediate or resistant)
With recognizing 3GC resistance, appropriate therapy should be selected based on local formulary and Antimicrobial Stewardship guidelines. At this point, an ESBL is evident and beta-lactam treatment options are likely limited to carbapenems. If a more specific antimicrobial therapy is desired, continue evaluation in Step 2.
Step 2: Review cefoxitin and cefepime susceptibilities to differentiate AmpC and ESBL.
A. Amp C
- Cefoxitin MIC 16 mcg/mL (intermediate or resistant) is indicative of presence of an AmpC. Although, a combination of an ESBL with significant porin restriction could present as cefoxitin resistant.
AND
- Cefepime MIC ≤2 mcg/mL (susceptible) reinforces the presumptive presence of an AmpC
B. AmpC and ESBL
- Cefoxitin I/R (MIC =>16 mcg/mL)
AND
- Cefepime I/R (MIC =>4 mcg/mL)
This pattern indicates that both mechanisms could be present, at this level the presence of the ESBL is more relevant from a therapeutic perspective since cefepime wouldn’t be an option.
C. ESBL
- Cefepime S (MIC ≤2)
AND
- Cefoxitin S (MIC ≤8)
This scenario is possible since some ESBL genotypes can have a low affinity against cefepime. By my own experience, we have around 44% of our ESBL being cefepime susceptible.
This differentiation of AmpC and ESBL is important as an AmpC carrying Enterobacterales may be treated with cefepime while ESBL carrying Enterobacterales likely requires a carbapenem or a beta-lactam alternative.
Enterobacterales (E. coli, K. pneumoniae, K. oxytoca, or P. mirabilis only):

Table 1 Note: This table is not intended to be a therapeutic guideline. It is to illustrate the different resistance patterns and the possible therapeutic option based on the spectrum of the beta-lactamase detected. S = susceptible, I = intermediate, R = Resistant.
5. Can SPiCE-M organisms carry an ESBL?
Yes, although it is important to always consider that SPiCE-M organisms to carry a chromosomal AmpC, they may also carry an ESBL as an acquired plasmid.
To evaluate for an ESBL in a SPiCE-M organism, review the cefepime MIC. A cefepime I/R (MIC 4) could indicate the presence of an ESBL along with the chromosomal AmpC.
It is important especially since the drug of choice for a wild-type SPiCE-M may be cefepime.
For long time, many Microbiology laboratories have only performed ESBL screening and confirmation by request. Proper screening and testing for ESBL is critical for both epidemiology and antimicrobial stewardship. A better understanding of the role of accurate and rapid identification of resistance mechanisms against beta-lactams facilitates use of more targeted antimicrobial therapy. It would allow us to make the best use for our current antimicrobials as well as find a better niche for the new agents along with new inhibitors with more potent and broader spectrum.
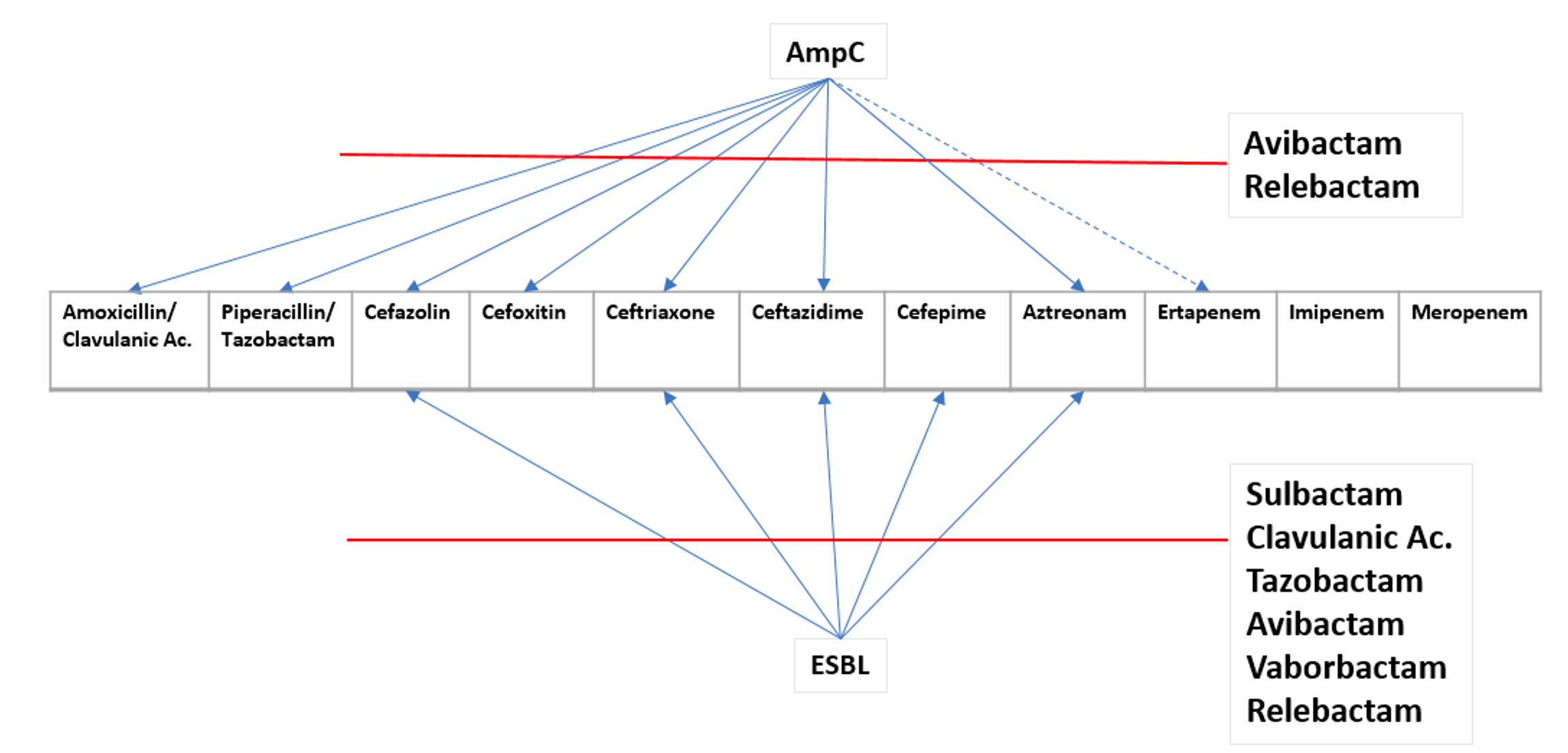
Figure 1. Spectrum of activity between ESBL Vs AmpC.
References & Readings
8. George A. Jacoby et al. AmpC β-Lactamases. Clinical Microbiology Reviews, Jan. 2009, p161-182. ASM
RECOMMENDED TO YOU

